Late-life depression remains among the most under-diagnosed health conditions in the developed world. This methodology paper describes how Verbasync transforms regular geriatric telephone companionship conversations into structured, clinically grounded signals anchored on GDS-15, GAD-7 and C-SSRS, with privacy-preserving outputs designed for professional caregivers and family members.
Abstract
Late-life depression remains among the most under-diagnosed health conditions in the developed world, despite well-established associations with functional decline, healthcare utilization, and mortality from suicide. The classical screening apparatus - periodic clinician-administered instruments such as the Geriatric Depression Scale - is constrained by clinical access, episodic measurement, and a documented insensitivity to the specific phenomenology of geriatric affective distress.
Verbasync operates an artificial intelligence companion that maintains regular voice conversations with older adults living at home or in residential care facilities. This paper describes the methodology by which that data is processed into structured, clinically grounded signals suitable for use by professional caregivers and family members.
We present the architecture of a multi-dimensional classification framework anchored on three validated geriatric instruments - GDS-15, GAD-7, and C-SSRS - and explain how the system operationalises eight dimensional axes, three independent safety flags, and a derived aggregate index. We discuss the geriatric-specific calibrations required to address known biases such as social desirability minimization, masked depression presentation, and the high prevalence of passive suicidal ideation in late life.
We outline the privacy architecture that allows clinically informative outputs to be delivered to care organisations under GDPR and HIPAA-equivalent frameworks without exposing private conversational content. Finally, we describe ongoing validation work and frame the limitations of the current system relative to the long-term ambition of producing a clinically validated decision-support tool.
Keywords: geriatric depression; suicide prevention; digital phenotyping; conversational AI; late-life affective disorders; telehealth; GDS-15; GAD-7; C-SSRS.
This white paper describes methodology and is not a clinical efficacy claim. The Verbasync mood-tracking framework is not a diagnostic instrument and is not a substitute for professional clinical assessment.
1. Introduction
Loneliness and social isolation among older adults are now widely recognised as a public health emergency in their own right. The meta-analytic work of Holt-Lunstad and colleagues has demonstrated that perceived social isolation confers a mortality risk of comparable magnitude to smoking, exceeding that of obesity and physical inactivity. In parallel, late-life depression is estimated to affect between five and ten percent of older adults at any given time at a major-disorder threshold, with subsyndromal presentations affecting an additional fifteen to thirty percent. Suicide in late life is a particular concern: in many high-income countries, men over the age of seventy-five exhibit the highest age-adjusted suicide rate of any demographic group.[1][2][3][4][5]
Despite this epidemiological weight, late-life depression is detected at rates that have remained stubbornly low across decades of primary-care research. Mojtabai and others have documented detection rates in primary care below fifty percent, with under-treatment of those who are detected. The most validated screening instrument in this population, the Geriatric Depression Scale, is administered episodically during clinical encounters and is therefore necessarily blind to the daily fluctuations and subtle symptomatic shifts that characterise the early phases of decompensation.[6][7][8]
Older adults frequently minimise distress when speaking with healthcare professionals, a phenomenon variously described in the literature as social desirability bias, stoic generation effects, or fear of being placed in residential care.
Verbasync operates a voice-based artificial intelligence companion that maintains regular telephone conversations with older adults, primarily in their own homes or in residential care facilities serviced by professional home-care providers and EHPADs. These conversations are intentionally informal: the system is not a clinical instrument and is not represented to users as such. Their role is companionship: to provide regular, warm, low-pressure interaction with someone who has time, attention, and continuity.
We have, however, observed across our operational history that these conversations contain a rich seam of clinically informative signal. Older adults speaking to a non-judgmental conversational partner over time disclose patterns - about sleep, engagement, social connection, and hope - that are difficult or impossible to elicit reliably during a fifteen-minute primary-care visit.
This paper describes the methodology by which Verbasync processes that conversational data into a structured, multi-dimensional snapshot of affective and psychological state. We focus on three contributions: the data-processing pipeline; the classification framework and its geriatric calibrations; and the privacy architecture that permits the output to be shared with caregivers and family members under European and North American regulatory frameworks.
We make no claim, in this paper or elsewhere, that the Verbasync system constitutes a diagnostic instrument. We do claim that it produces a structured, reproducible, and clinically informed signal - one that can support the work of trained professionals and concerned family members in identifying older adults who may benefit from a more thorough clinical evaluation.
2. Clinical Background
2.1 The phenomenology of late-life depression
Depression in older adults is, in important respects, not the same illness as depression in younger populations. The criterion-set of the DSM was developed largely on adult samples in which expressed sadness, hopelessness, and suicidal ideation were the dominant features. Geriatric depression more often presents through somatic complaints, anhedonia, apathy, irritability, executive dysfunction, and a constellation of symptoms that Alexopoulos and others have characterised as the depression-executive dysfunction syndrome of late life.[4][9]
This phenomenological divergence has direct measurement consequences. Standard depression instruments calibrated on younger populations exhibit reduced sensitivity in the elderly; the GDS was developed precisely to address this gap by removing somatic items that perform poorly in a population in whom routine somatic complaints carry weak diagnostic specificity. The fifteen-item version of the GDS has accumulated extensive validation evidence and is now among the most widely used screening instruments in geriatric practice.[10][11][12][13]
Several specific features of late-life depression matter for the design of any conversational assessment system. First, masked depression - a clinical presentation in which the depressive disorder manifests primarily through somatic, cognitive, or behavioural symptoms rather than through expressed sadness - is unusually common in older adults. Second, anhedonia and apathy function as core markers in this population, often more reliably than reported sadness. Third, hopelessness and reduced future-orientation are among the strongest predictors of suicide in late life.[4][14][15][16]
2.2 Suicide in late life
The work of Conwell and colleagues established the contemporary understanding of late-life suicide as a clinical entity distinct from suicide in younger adults. Older adults who die by suicide have higher rates of medical comorbidity, lower rates of communicated intent, more lethal means selection, and more frequent expression of passive rather than active ideation in the period preceding the act.[5][17]
The Interpersonal Theory of Suicide identifies perceived burdensomeness and thwarted belongingness as proximal psychological constructs that connect late-life social circumstances to suicide risk. The Columbia Suicide Severity Rating Scale is the most widely adopted clinical instrument for stratifying suicidal ideation and behaviour. Its three-tier characterisation of ideation - none, passive, active - and its distinction between ideation, plan, intent, and behaviour provide a tractable conceptual scaffold for surfacing safety-relevant signal from naturalistic interaction data.[18][19][20]
2.3 Anxiety, social connection, and dimensional measurement
Anxiety in older adults is highly comorbid with depression and contributes independently to functional decline. The GAD-7 is the standard brief instrument for anxiety symptomatology and complements the GDS in capturing the affective spectrum.[21][22]
Social connection has progressed in the last decade from a soft psychosocial variable to a measurable predictor of physical health outcomes. In addition to the meta-analytic evidence on mortality risk, objective social isolation and subjective loneliness have each been associated with cognitive decline, cardiovascular morbidity, and accelerated immunosenescence.[1][2][23]
Across these domains, the contemporary clinical research literature is converging on the value of dimensional over categorical measurement. Single-label classifications compress a clinically rich phenomenon into a binary that obscures both severity and the specific symptom profile driving impairment. Dimensional approaches preserve more of the underlying signal and align better with how clinicians actually reason about cases. The Verbasync framework is designed in this dimensional spirit.[24]
3. System Overview
The Verbasync mood-tracking module is a downstream component of a broader voice-companion platform. Older adults interact with the platform via standard telephone calls, typically between five and twenty minutes in duration, scheduled at intervals appropriate to their preferences and care plan. Conversations are conducted with full informed consent, with the system identifying itself transparently and offering an explicit opt-out at every interaction.
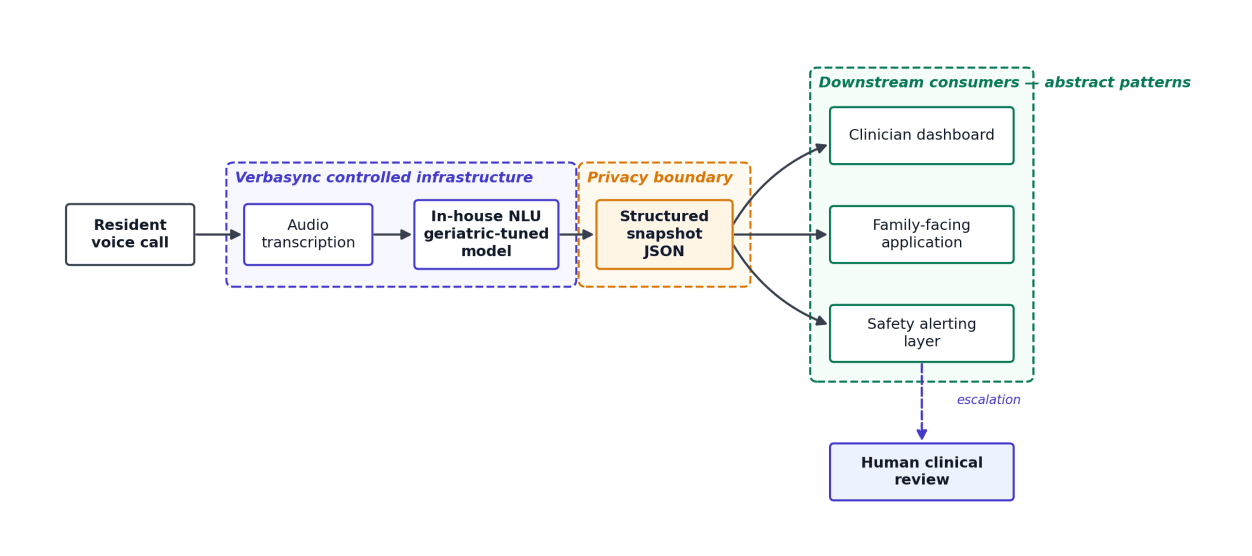
After each call, the audio is transcribed and the resulting text is processed by an internal natural-language understanding system. This system is an in-house deployment of an open-weights foundation model further trained on geriatric conversational data, clinical case material, and structured exemplars annotated according to the framework described in this paper.
Operating an internal model is a deliberate choice driven by three constraints: data sovereignty, clinical specialisation, and reproducibility. Resident speech does not leave Verbasync controlled infrastructure; the model is calibrated to older-adult populations in French and English; and model behaviour is locked to specific weights under version control rather than being subject to silent updates.
The output of the natural-language processing stage is a structured snapshot - a JSON object - representing the multi-dimensional clinical state inferred from the conversation. This snapshot feeds a clinician-facing dashboard, a family-facing application, and an internal alerting layer that escalates safety-critical signals to human review. The snapshot is the boundary at which abstract, privacy-safe clinical information replaces raw conversational content.
4. Data Processing Pipeline
The pipeline applies a deterministic sequence of steps to each transcript. Each step is auditable, versioned, and observable.
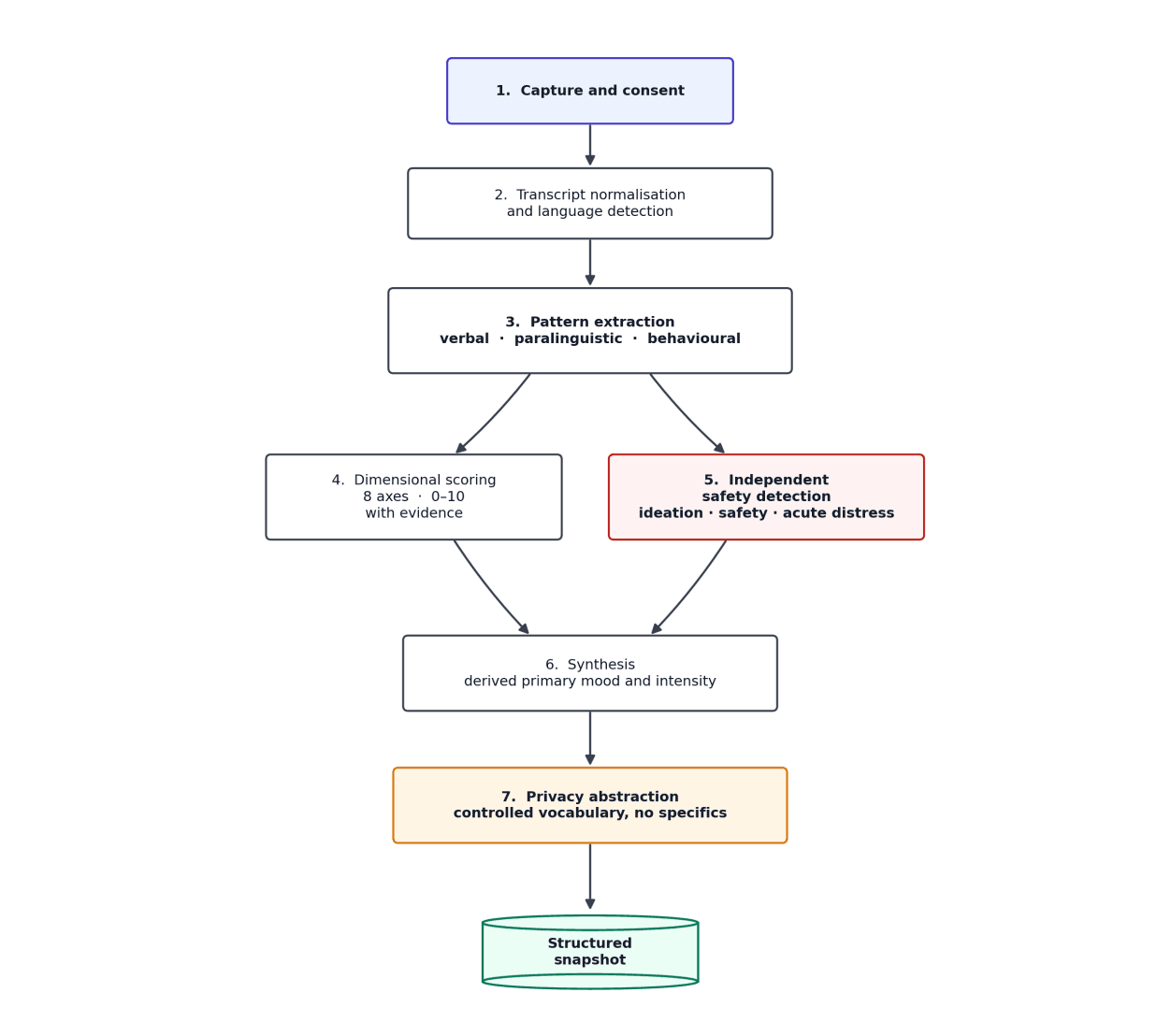
4.1 Capture and consent
Calls are initiated only after explicit informed consent, refreshed at appropriate intervals according to local regulatory frameworks. The system identifies itself as an artificial intelligence at every call, and pauses or terminates the conversation on request. Audio is processed transiently for transcription and is not retained beyond the operational window required to produce the structured snapshot.
4.2 Transcript normalisation and language detection
The raw transcript undergoes a normalisation pass that handles disfluencies, transcription artefacts, and turn-taking annotation. The system operates natively in French and English; language is detected at this stage and propagated through the downstream pipeline so that all linguistic markers, output text, and free-form clinical evidence are produced in the resident's language of conversation.
4.3 Pattern extraction
Before any scoring is attempted, the system extracts patterns at three distinct levels of analysis. Verbal patterns capture content-bearing features of the resident's speech: minimisation of difficulties, low future-orientation, absence of pleasure references, repeated self-deprecation, and related signals. Paralinguistic patterns capture pauses, hesitations, sighs, and voice qualities when recoverable. Behavioural patterns capture topic avoidance, abrupt shifts, withdrawal, contradictions, and refusal to elaborate.
This pattern-extraction step exists for two reasons. First, it forces the system to ground subsequent scoring in observable interactional features rather than inferred internal states. Second, it produces an audit trail that allows trained reviewers to retrospectively assess whether the dimensional scores are warranted by the underlying observations.
4.4 Dimensional scoring
The eight clinical dimensions described in Section 5 are scored on a zero-to-ten scale, with explicit behavioural anchors at the extremes and midpoint. Each dimensional score is accompanied by a brief, privacy-safe evidence statement explaining the basis for the score in clinical-pattern terms. The scoring step is constrained to produce no score without evidence and no evidence that violates the privacy contract.
4.5 Independent safety detection
Critical safety flags - passive or active suicidal ideation, safety concerns suggesting mistreatment or neglect, and acute distress states - are detected through a path that operates independently of the dimensional scores. This separation is intentional. Dimensional scoring captures continuous variation in mood, anxiety, and engagement; safety detection captures categorical, action-relevant states that demand immediate attention regardless of the dimensional profile.
4.6 Synthesis and aggregate index
A derived primary mood label and intensity, on a scale aligned with the existing care-organisation dashboard taxonomy, is computed from the dimensional profile and safety flags via a deterministic mapping. This aggregation exists for backwards compatibility with existing visualisation and alerting systems; the underlying dimensional profile remains the canonical representation of the conversation's clinical content.
4.7 Privacy abstraction
Every free-text field in the snapshot is constrained, at the source, to abstract clinical pattern descriptions. Names, specific events, specific medical conditions or medications, specific places, and verbatim quotations are excluded by design from the snapshot itself, not merely redacted afterwards. The privacy contract is enforced at the moment of generation, not as a downstream filter that could fail open.
5. Classification Framework - The Eight Dimensions
The Verbasync framework scores eight dimensions, each on a zero-to-ten scale where higher scores represent greater clinical concern. The dimensions are not independent in a statistical sense, but they are conceptually distinct and were chosen to map onto the validated symptom clusters of GDS-15, GAD-7, and clinical observation traditions.[11][12][22]
We have intentionally limited the system to eight dimensions rather than attempting to capture every clinically relevant axis. Each additional dimension introduces measurement noise; each one removed loses signal. The eight retained here represent the minimum sufficient set for capturing clinically actionable variation observed in typical companionship calls.
| # | Dimension | Primary anchoring | Core clinical role |
|---|---|---|---|
| 1 | Mood affect | GDS-15 items 5, 7, 11 | Prevailing affective tone; sustained sadness vs flat vs warm |
| 2 | Anhedonia / apathy | GDS-15 items 2, 3, 4, 13 | Loss of interest and pleasure; primary marker of masked depression |
| 3 | Anxiety | GAD-7; GDS-15 item 6 | Generalised worry, restlessness, somatic anxiety |
| 4 | Hopelessness / futurity | GDS-15 items 8, 14 | Future orientation; strongest single predictor of late-life suicide |
| 5 | Social connection | GDS-15 items 9, 15 | Quality and quantity of human connection; isolation marker |
| 6 | Self-worth | GDS-15 item 12 | Worthlessness, burden ideation; proximal trigger for suicide risk |
| 7 | Somatic burden | Direct observation | Distress-laden somatic complaints, calibrated against geriatric baseline |
| 8 | Cognitive signals | GDS-15 item 10; observation | Coherence, word-finding, orientation; gates reliability of the others |
5.1 Mood affect
Captures the prevailing affective tone of the conversation. Mapped onto GDS items 5, 7, and 11. Anchored at zero by clear positive affect and explicit expressions of warmth or satisfaction; at five by flat affect; at ten by pervasive sadness or despair across the conversation. A brief low-affect moment within an otherwise warm conversation does not dominate the score; sustained presence does.
5.2 Anhedonia and apathy
The single most important marker of masked depression in late life. Mapped onto GDS items 2, 3, 4, and 13. Captures loss of interest, pleasure, and engagement through references to abandoned activities, the absence of pleasure references where they would be expected, and descriptions of reduced energy. The framework treats anhedonia as a primary signal rather than a secondary one.[4][15]
5.3 Anxiety
Mapped onto GAD-7 and GDS item 6. Captures expressed worry, restlessness, and somatic anxiety markers. The dimension is sensitive to generalised anxious tone across topics rather than to the brief mention of a single specific concern, which in the geriatric context often reflects realistic appraisal rather than anxious symptomatology.
5.4 Hopelessness and futurity
Captures the resident's orientation toward the future. Mapped onto GDS items 8 and 14. This dimension carries particular clinical weight because hopelessness has been identified as among the strongest single predictors of completed suicide in late life. A resident with low expressed sadness but a profound absence of future-orientation should be considered clinically concerning.[16][18]
5.5 Social connection
Captures the quality and quantity of social engagement evident in the conversation. Mapped onto GDS items 9 and 15. Higher scores indicate greater isolation. The dimension carries an important nuance specific to residential care: when a resident has a warm, regular relationship with professional caregivers but is otherwise isolated from family and friends, the score is capped to reflect that some meaningful human contact is preserved.
5.6 Self-worth
Captures the resident's expressed sense of self-worth, contribution, and identity. Mapped onto GDS item 12. Severe scores are clinically concerning in their own right and also operate as a proximal trigger for suicide risk via the burden-ideation pathway described in the Interpersonal Theory of Suicide. Profound expressions of worthlessness or being a burden are independently flagged in the safety-detection layer.[18][19]
5.7 Somatic burden
Captures the intensity and prominence of physical complaints. The dimension exists because somatic content is highly informative in a geriatric population but must be interpreted carefully. The framework anchors the geriatric baseline - matter-of-fact mention of chronic somatic conditions - at a low score, reserving higher scores for complaints that are sustained, distressed, or impair daily functioning.
5.8 Cognitive signals
Captures observable cognitive function during the conversation: coherence, word-finding, orientation, and in-conversation repetition. Mapped onto GDS item 10 and direct observation traditions. The framework downweights the reliability of the other dimensions when this dimension scores high, on the principle that verbal expression maps less cleanly onto internal state when significant cognitive impairment is present.
6. Critical Safety Detection
Independent of dimensional scoring, the system runs a dedicated safety-detection pass over each transcript. This pass produces three categorical outputs.
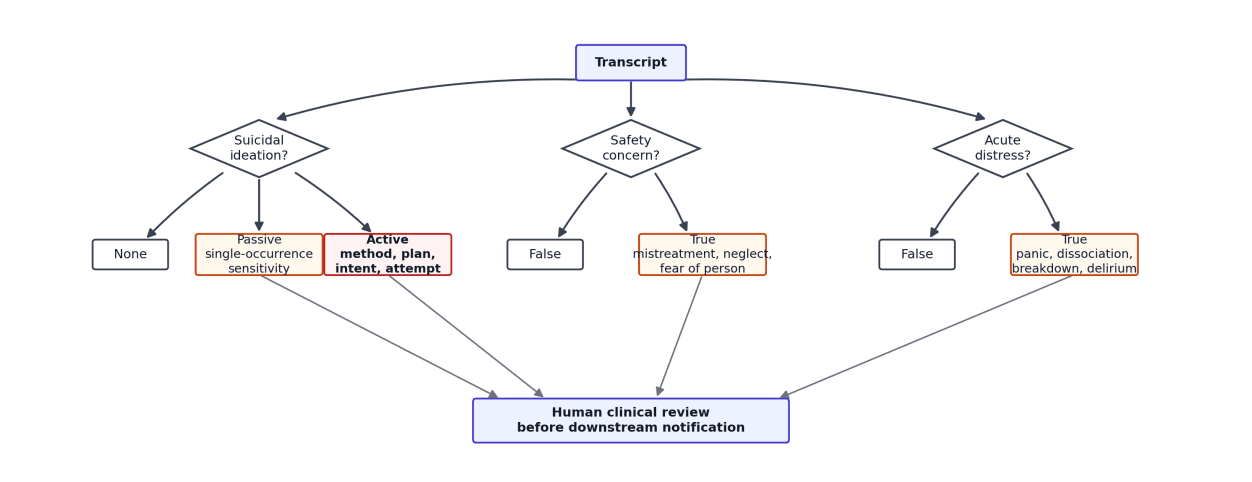
6.1 Suicidal ideation
The framework adopts the three-tier characterisation of the C-SSRS: none, passive, active. The clinical literature on late-life suicide demonstrates that older adults express ideation passively far more often than actively in the period preceding suicide. Phrases that signal a wish to die, a sense that one has lived long enough, expressions of being a burden, or passive waiting for the end are flagged as passive ideation even on a single occurrence within a conversation. Active ideation - method, plan, intent, timing, or recent attempt - is flagged separately and triggers immediate escalation.[5][17][20]
The single-occurrence sensitivity of the passive-ideation flag is deliberate. The clinical cost of a false negative in this domain is severe and asymmetric to the cost of a false positive. False positives are managed downstream through human review by trained care staff before any communication reaches family members.
6.2 Safety concern
A boolean flag is set true when the conversation contains patterns suggestive of mistreatment, neglect by caregivers or family, refusal of essential care that endangers the resident, or expressed fear of a specific person in the resident's environment. This is a B2B-critical signal because institutional clients have both regulatory obligations and operational interest in early identification of these situations.
6.3 Acute distress
A boolean flag is set true when the conversation evidences active panic, dissociation, an extreme emotional breakdown during the call itself, an acute confusional state suggesting delirium, or a recent unresolved acute medical event. These states demand same-day clinical attention and are escalated accordingly.
The evidence statements accompanying each flag are constrained, like all free-text fields, to abstract clinical pattern descriptions. A passive ideation flag might read "multiple passive ideation markers detected, including burden ideation and existential disengagement"; it would never include the verbatim phrasing from the conversation that triggered detection.
7. Geriatric-Specific Calibrations
A general-purpose affective classification system applied naively to geriatric conversation will fail in characteristic ways. The framework applies several calibrations to address documented failure modes.
| Calibration | Failure mode addressed | Mechanism |
|---|---|---|
| Somatic baseline | Inflation of negative-mood scores by routine somatic talk | Matter-of-fact health mentions anchored at low somatic-burden score; no spillover to mood-affect or hopelessness |
| Social desirability bias | Direct affirmations masking underlying distress | Detection of hesitation, sighs, contradictions, formulaic responses; indirect cues weighted over direct affirmations |
| Masked depression cluster | Depression presenting without expressed sadness | Co-occurring anhedonia, somatic burden, withdrawal, and reduced affect scored as depressive even absent sadness vocabulary |
| Hostility override | Engaged-sounding but interpersonally negative conversations misclassified as positive | Sustained hostility forces negative primary-mood classification regardless of dimensional aggregation |
| Cognitive caveat | Verbal expression less reliable when cognitive impairment is present | High cognitive-signals score downweights all other dimensions and routes for human review |
7.1 The somatic baseline
Older adults discuss health, medications, and minor physical difficulties as a routine feature of conversation. Naive systems consistently inflate negative-mood classifications on the basis of routine somatic content that carries no clinical valence in context. The framework anchors brief, matter-of-fact somatic mentions at a low somatic-burden score and prevents this content from inflating mood-affect or hopelessness dimensions.
7.2 Social desirability bias
The geriatric assessment literature has long documented social desirability bias as a prevalent systematic distortion in elderly self-report. Older adults reliably respond "I am fine" or "ca va" to direct questions about well-being even when distressed. The framework detects hesitated affirmations, sighs, topic shifts, contradictions, and repeated formulaic responses; when these are detected, indirect cues are weighted more heavily than direct affirmations.[25][26]
7.3 The masked depression cluster
The framework actively monitors for co-occurrence of anhedonia, somatic complaints, social withdrawal, and reduced affect - the classical masked-depression cluster. When this cluster is observed, relevant dimensions are scored at moderate-to-high levels even in the absence of explicitly named sadness.[4][9]
7.4 The hostility override
Sustained hostility, anger, or insulting behaviour toward the conversational partner is treated as overriding dimensional aggregation logic and forcing a negative primary-mood classification. This prevents superficially active or engaged conversations with strongly negative interpersonal valence from being misclassified as positive.
7.5 The cognitive caveat
When the cognitive-signals dimension scores high, the framework downweights the reliability of every other dimension and notes the situation in the data-quality field. Elevated cognitive-signal conversations are flagged for human clinical review and are not used to drive automated alerting downstream.
8. Privacy and Compliance Architecture
The Verbasync mood tracker operates in a regulatory environment that combines the requirements of the European General Data Protection Regulation, which classifies health and mental-health data as special-category personal data under Article 9, with HIPAA-equivalent frameworks in the United States.[33][34]
The architectural response rests on a single principle: detection is specific; reporting is abstract. The internal processing layer operates on full transcript content and identifies specific linguistic markers. The output layer - the snapshot that crosses into storage and human-facing dashboards - is constrained to contain no verbatim quotations, no personal names, no specific events, no specific medical conditions or treatments, no specific places, and no identifying timeframes.
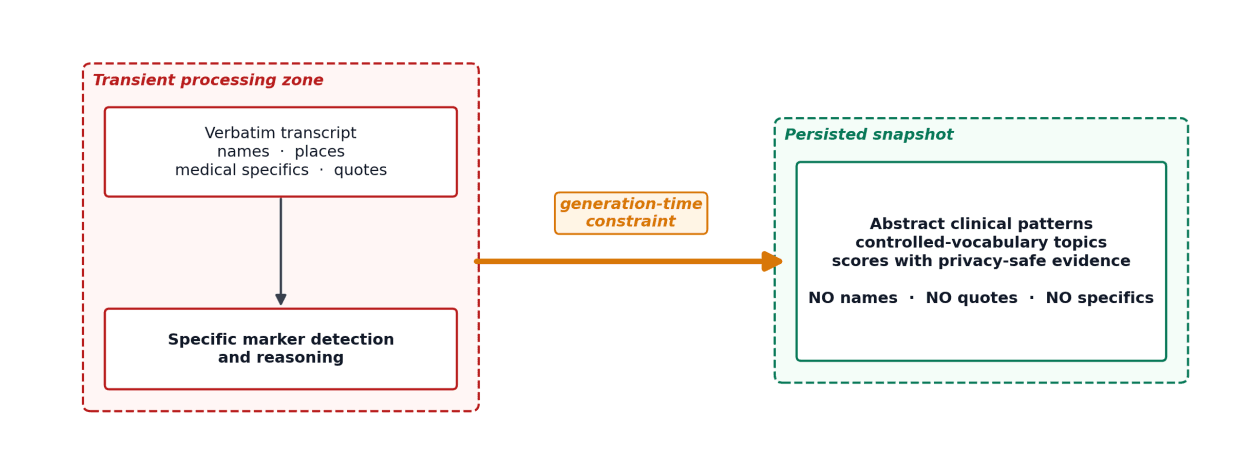
This is not a downstream redaction layer. It is a constraint enforced at the moment of generation. The framework does not produce a richer output that is then filtered; it produces the abstract output directly. This reflects a security-engineering principle: filters fail open, while constructive constraints fail closed.
A second pillar of the privacy architecture is the use of a controlled vocabulary for conversation topics. Rather than allowing free-text topic tagging, which would reproduce conversational specifics in the snapshot, the framework selects from a fixed taxonomy of general categories such as Health and Wellness, Family Connection, Caregiver Relationship, and Emotional Hardship. This taxonomy provides clinical and operational signal without permitting the leak of personal specifics.
A third pillar is data sovereignty at the model layer. The natural-language understanding stage operates on Verbasync controlled infrastructure rather than via third-party APIs; resident speech does not leave Verbasync's environment. We make no claim that this architecture eliminates all privacy risk. We do claim that it represents a principled response to the regulatory landscape.
9. Validation Strategy
The validation programme for the Verbasync mood-tracking framework is structured around four converging strands, conducted in collaboration with institutional partners.
The first strand is inter-rater reliability between the framework's outputs and the judgements of trained clinical reviewers. This work is conducted on samples of anonymised conversations, with reviewers blinded to framework outputs and producing independent dimensional and flag-level judgements. Agreement is measured using standard reliability statistics and stratified by conversation length, cognitive-signal level, and language.
The second strand is convergent validity with periodic clinician-administered GDS-15 assessments. A subset of consenting residents complete the GDS-15 with their care provider at defined intervals, and we examine correspondence between the framework's longitudinal dimensional profile in the surrounding period and the GDS-15 score.
The third strand is discriminant validity: the framework's ability to differentiate residents whose dimensional profiles diverge in clinically meaningful ways and to track within-resident change over time. Cross-sectional differentiation is necessary but not sufficient; longitudinal sensitivity to clinically meaningful change is the more demanding test.
The fourth strand is clinical outcome correlation: the extent to which the framework's signals, particularly safety flags, correlate with clinical events recorded by institutional partners in the period following the conversation. This is rigorous and operationally challenging, requiring careful attention to confounding by the very interventions that the system is designed to trigger.
We anticipate publishing the results of these validation strands in peer-reviewed venues as the data matures.
10. Limitations
First, the framework produces a snapshot per conversation, not a longitudinal trajectory relative to a per-resident baseline. The clinical interpretation of any single snapshot is necessarily limited. A low-affect day in a baseline-low-affect resident carries different meaning than the same snapshot in a previously bright-affect resident. The trajectory layer is a planned future development, requiring four to six weeks of per-resident history to be clinically meaningful.
Second, the framework relies on verbal expression. Residents with severe expressive aphasia, severe cognitive impairment, or severe sensory deficits that disrupt conversation are not well served by this approach; the cognitive-caveat downweighting is a partial mitigation but not a substitute for alternative assessment modalities.
Third, the framework has been developed and calibrated in French and English. Cross-linguistic and cross-cultural extension is non-trivial; idioms of distress, cultural norms around emotional expression, and the specific vocabulary of suicidal ideation vary substantially across cultures.
Fourth, and most importantly: the framework is not a clinical instrument and must not be represented as one. It is a structured signal designed to support trained professionals and concerned family members in identifying older adults who may benefit from a more thorough clinical evaluation. The framework's outputs do not replace clinical assessment, do not constitute diagnosis, and should not drive consequential clinical decisions in isolation.
11. Conclusion
We have described the methodology by which Verbasync transforms naturalistic geriatric telephone conversations into structured, clinically grounded snapshots of affective and psychological state. The framework is anchored on validated geriatric instruments, calibrated for the specific phenomenology of late-life affective distress, structured around eight dimensional axes and three independent safety flags, and designed within a privacy architecture that meets the requirements of the European and North American regulatory environments in which we operate.
We believe that the systematic application of clinically grounded methodology to the rich data stream produced by consensual, regular conversational engagement with older adults represents a meaningful complement to the episodic clinical assessment that constitutes the existing standard of care. We do not believe it represents a replacement, and we are committed to the rigorous validation work necessary to clarify exactly what role this class of signal can play in the broader ecology of geriatric mental healthcare.
We welcome dialogue with clinical researchers, geriatricians, and care-organisation leaders interested in collaborating on the validation programme described in Section 9, and on the broader question of how digital companionship platforms can be made not only kind to the older adults they serve but clinically useful to the professionals charged with their care.
Correspondence: Alain Briez, Verbasync - contact@verbasync.com.
References
- [1] Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: a meta-analytic review. PLoS Medicine. 2010;7(7):e1000316..
- [2] Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspectives on Psychological Science. 2015;10(2):227-237..
- [3] Blazer DG. Depression in late life: review and commentary. Journals of Gerontology Series A. 2003;58(3):249-265..
- [4] Alexopoulos GS. Depression in the elderly. Lancet. 2005;365(9475):1961-1970..
- [5] Conwell Y, Van Orden K, Caine ED. Suicide in older adults. Psychiatric Clinics of North America. 2011;34(2):451-468..
- [6] Mojtabai R. Diagnosing depression in older adults in primary care. New England Journal of Medicine. 2014;370(13):1180-1182..
- [7] Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, Leirer VO. Development and validation of a geriatric depression screening scale: a preliminary report. Journal of Psychiatric Research. 1982-83;17(1):37-49..
- [8] Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clinical Gerontologist. 1986;5(1-2):165-173..
- [9] Alexopoulos GS, Meyers BS, Young RC, Kakuma T, Silbersweig D, Charlson M. Clinically defined vascular depression. American Journal of Psychiatry. 1997;154(4):562-565..
- [10] Mitchell AJ, Bird V, Rizzo M, Meader N. Diagnostic validity and added value of the Geriatric Depression Scale for depression in primary care: a meta-analysis of GDS30 and GDS15. Journal of Affective Disorders. 2010;125(1-3):10-17..
- [11] Almeida OP, Almeida SA. Short versions of the geriatric depression scale: validity for diagnosis of a major depressive episode according to ICD-10 and DSM-IV. International Journal of Geriatric Psychiatry. 1999;14(10):858-865..
- [12] Burke WJ, Roccaforte WH, Wengel SP. The short form of the Geriatric Depression Scale: a comparison with the 30-item form. Journal of Geriatric Psychiatry and Neurology. 1991;4(3):173-178..
- [13] Greenberg SA. The Geriatric Depression Scale (GDS). Best Practices in Nursing Care to Older Adults. The Hartford Institute for Geriatric Nursing. 2012..
- [14] Gallo JJ, Rabins PV. Depression without sadness: alternative presentations of depression in late life. American Family Physician. 1999;60(3):820-826..
- [15] Pizzagalli DA. Depression, stress, and anhedonia: toward a synthesis and integrated model. Annual Review of Clinical Psychology. 2014;10:393-423..
- [16] Beck AT, Brown G, Berchick RJ, Stewart BL, Steer RA. Relationship between hopelessness and ultimate suicide: a replication with psychiatric outpatients. American Journal of Psychiatry. 1990;147(2):190-195..
- [17] Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biological Psychiatry. 2002;52(3):193-204..
- [18] Joiner TE. Why People Die by Suicide. Cambridge, MA: Harvard University Press; 2005..
- [19] Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE Jr. The interpersonal theory of suicide. Psychological Review. 2010;117(2):575-600..
- [20] Posner K, Brown GK, Stanley B, Brent DA, Yershova KV, Oquendo MA, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies. American Journal of Psychiatry. 2011;168(12):1266-1277..
- [21] Lenze EJ, Mulsant BH, Shear MK, Schulberg HC, Dew MA, Begley AE, et al. Comorbid anxiety disorders in depressed elderly patients. American Journal of Psychiatry. 2000;157(5):722-728..
- [22] Spitzer RL, Kroenke K, Williams JBW, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine. 2006;166(10):1092-1097..
- [23] Crooks VC, Lubben J, Petitti DB, Little D, Chiu V. Social network, cognitive function, and dementia incidence among elderly women. American Journal of Public Health. 2008;98(7):1221-1227..
- [24] Insel TR, Cuthbert BN. Brain disorders? Precisely. Science. 2015;348(6234):499-500..
- [25] Stoyanova MS, Hope DA. Gender, gender roles, and anxiety: perceived confirmability of self report, behavioral avoidance, and physiological reactivity. Journal of Anxiety Disorders. 2012;26(1):206-214..
- [26] Soubelet A, Salthouse TA. Influence of social desirability on age differences in self-reports of mood and personality. Journal of Personality. 2011;79(4):741-762..
- [27] Heisel MJ, Flett GL. The development and initial validation of the geriatric suicide ideation scale. American Journal of Geriatric Psychiatry. 2006;14(9):742-751..
- [28] Mohr DC, Zhang M, Schueller SM. Personal sensing: understanding mental health using ubiquitous sensors and machine learning. Annual Review of Clinical Psychology. 2017;13:23-47..
- [29] Insel TR. Digital phenotyping: a global tool for psychiatry. World Psychiatry. 2018;17(3):276-277..
- [30] Cummins N, Scherer S, Krajewski J, Schnieder S, Epps J, Quatieri TF. A review of depression and suicide risk assessment using speech analysis. Speech Communication. 2015;71:10-49..
- [31] Levy BR. Stereotype embodiment: a psychosocial approach to aging. Current Directions in Psychological Science. 2009;18(6):332-336..
- [32] Pinto-Meza A, Serrano-Blanco A, Penarrubia MT, Blanco E, Haro JM. Assessing depression in primary care with the PHQ-9: can it be carried out over the telephone? Journal of General Internal Medicine. 2005;20(8):738-742..
- [33] European Parliament and Council. Regulation (EU) 2016/679 (General Data Protection Regulation), Article 9 - Processing of special categories of personal data. Official Journal of the European Union. 2016..
- [34] United States Department of Health and Human Services. Health Insurance Portability and Accountability Act of 1996, Privacy Rule. 45 CFR Part 160 and Subparts A and E of Part 164..